John Galt Is Impotent In A Pandemic
Discontinuity.
Abrupt change.
Collapse.
Chaos.
Whatever term you might choose to use, there’s no disputing that if the epidemiologists are correct, the COVID-19 pandemic will be the largest, most impactful world event since 9/11. How we respond to the pandemic will define our society, likely for generations to come.
The response to 9/11 was close to exactly the opposite of what I would consider best. Instead of asking why small groups of people felt so ostracized and minimized that violence was their last resort and then acting to address the root causes, the US chose to demonize and further ostracize Muslims in generally, thereby creating a much larger and endless supply of new terrorists to fight. Over a million people died, many more millions were displaced and an entire generation of US military lives were wasted. But a handful of people got filthy rich off it.
The business and political worlds of today live for these discontinuities. Back when I was running an agricultural biotechnology startup, we were instructed that Monsanto and their spin-offs were so successful because they stood ready to respond to market discontinuities in their areas of operation. Regular, 1-3% annual changes in markets were for chumps. Giant change is what mattered, and so be it if mom and pop seed operations were obliterated by consolidating the entire seed industry. Likewise, in business generally in that era, the rise of the big box store was seen as a John Galt-like hero development as the parasitic small stores disappeared. Today, Big Bezos seems to be feasting off even those big boxes.
On the political front, Naomi Klein laid out in excruciating detail in Shock Doctrine how various disasters have been exploited by the political class to advance the interests of the oligarchy. Both civil rights and economic opportunity for huge portions of the population have been eroded.
Naomi Wolf warned us a few days ago to be on guard against deterioration of our rights in the COVID-19 outbreak:
As coronavirus spreads I just want to remind everyone to be on guard agains power grabs against civil liberties, using virus as rationale. “Never waste a good crisis” to mask the advance an otherwise unacceptable agenda, is the silent mantra of many political leaders.
— Dr Naomi Wolf (@naomirwolf) March 4, 2020
Today, CNN reports on ongoing discussions between the Trump Administration and the airline industry. It appears that at least some in the industry are concerned that data collection being demanded under a public health guise will be used “for other purposes”:
The US aviation industry and the Trump administration are in a pitched battle over the response to the coronavirus pandemic, three sources familiar with recent calls between officials from several government agencies and US airlines have told CNN.
In a series of contentious conversations, agency officials and aviation executives have clashed over the administration’s demand that airlines collect new kinds of data from passengers to help officials track potential virus carriers.
Okay, on the surface, I’m all for public health officials being able to access information quickly on who was sitting near whom on a flight with an infected person and quickly contact those who need to self-quarantine and get tested. But how do we make sure that data doesn’t wind up being misused? Also, it appears that the Trump Administration also wants the airlines to collect information on recent other travel by passengers:
This industry official says it took the US aviation industry two years to meet post-9/11 requirements, which also involved data collection.
Airlines are concerned that the Federal Register gives no clear end date on the data collection and worry that the US government could continue forcing them to collect it “for other purposes.”
“It seems they want us to do this for forever and we are pushing back,” the first source familiar said. The airlines — particularly their lawyers — are worried about what Customs and Border Protection officials will do with the information.
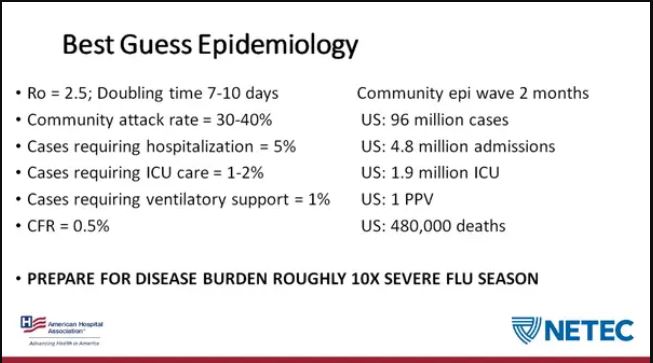
But what of the COVID-19 disruption? Rayne’s post yesterday provided much of the stark data. This tweet thread from Eli Pariser even goes so far as to suggest that we are just days away from the point at which Italy shut down large regions:
Here’s what the last 5 days of #COVID19US growth look like mapped to the Italian epidemic starting 2/22. Trajectory looks awful similar. pic.twitter.com/JvMcVZOlpA
— Eli Pariser (@elipariser) March 9, 2020
It’d be Day 15 on this chart.
— Eli Pariser (@elipariser) March 9, 2020
When hospitals are completely overwhelmed, there will be no Galt’s Gulch where heroes can wait out the outbreak. If we really see 20, 30 or even more than 50% of the global population being infected, the concept of isolation breaks down. No heroic action can be taken, because every single individual will be at risk for infection.
This impotence against the virus is because public health, in the end, is a social exercise. Will the outbreak become the discontinuity needed to convince the US to join the rest of the civilized world in making health care a social effort rather than a perk reserved for the very rich? If this doesn’t do it, it’s hard to imagine how it will ever happen.