(Not) Home for Christmas
[NB: check the byline, thanks. /~Rayne]
For the first time since he was in the service in the 1950s, my father may not be home for Christmas.
He was admitted to the hospital last week after experiencing complications related to chemotherapy. While his doctors are trying to work out a way to continue to treat him and release him, it’s likely he won’t be discharged on or before Christmas Day.
It’s difficult to feel hopeful right now; I know my dad is aware of the odds because he reminded me of the statistics for pancreatic cancer when I last spoke with him.
He’s done well up to now, more than two years since his diagnosis. The original cancer was knocked out by radiation therapy. The first round of chemo also worked well. But this cancer is stubborn and his numbers didn’t look good after a blood test earlier this year, so back into chemo he went.
But now it’s the chemo damaging him more than the cancer. I won’t go into specifics but the reason he’s in the hospital now isn’t because of the cancer but because of the therapy.
There’s no other effective alternate therapy, either.
The cost is staggering, too. I don’t know how much Medicare and his insurance are covering, but at tens of thousands of dollar per infusion, chemo is going to eat his life savings. The odds of survival for pancreatic cancer are poor but some of the odds are certainly shaped by patients’ financial ability to fight the disease.
We went through this last year when my father-in-law died after a five-year battle with a different cancer. He was left nearly bankrupt. In his case there were two immunotherapies employed over five years, and they were effective just as long as his oncologist said they would be, almost to the month. He died of congestive heart failure which may or may not have been caused by his cancer since his other siblings also died of congestive heart failure in the absence of cancer.
My father-in-law only had to fight the cancer and his genetics.
My dad, however, has to deal with betrayal on top of cancer.
When I spoke with my dad we also discussed therapies – there aren’t any, really, just the radiation and chemo he’s had to date. If there were effective immunotherapies we would have explored them but there aren’t any. Nor will an mRNA vaccine for pancreatic cancer arrive soon to help my dad’s immune system fight the cancer on its own.
There won’t be any soon under the Trump administration with Robert F. Kennedy Jr. helming Health and Human Services. All cancer research has been affected but cancers without immunotherapies or other effective alternatives to radiation and chemotherapy are those most in need of mRNA vaccine research.
RFK Jr. has assured disruption to all, and discouraged researchers so much that many have left the U.S. to continue work abroad. The cuts to federal funding will suppress investment by other parties. The damage to the U.S. as a center for cancer and vaccine research will last long beyond Trump’s term in office.
It will last beyond my dad’s likely lifetime which will not receive the benefit of research in progress but throttled under Trump and RFK Jr.
It has to be utterly gutting to my dad who’s been a lifelong Republican voter to know the party to which he has been so loyal has been savaging public health at a time when he is most vulnerable and needs it the most — a betrayal unto death. Though we’ve discussed them before I haven’t and won’t ask him about the GOP or Trump because my dad doesn’t need the additional aggravation.
But Dad did touch on RFK Jr., condemning him in his tersest fashion.
My dad doesn’t swear often. Very rarely, usually when he’s injured himself or something has broken during a repair he might muster a muttered “Damn!” or “Shit.” I am so not like my dad.
I do not ever recall him dropping an F-bomb. Again, I am so not like my dad.
My dad could be the image used in the meme of the Asian father – the stern face demanding more of progeny. He asked a lot of us, but then to not ask a lot would have been a failure on his part. He came from humble origins; he was dirt poor, the first in his family to go to college. He chose from one of two universities based on the entrance fee he could afford. Dad managed to earn a bachelor’s and master’s degree in engineering and raise a family, each of whom went to college. His experience assured him that we were wholly capable of reaching his expectations.
With this lifelong experience I didn’t expect to hear my dad swear about RFK Jr.’s gross mismanagement of HHS.
Instead my dad tsk-tsked and called RFK Jr. incompetent.
I wish I could convey the sensation of a mic drop at this point. In my dad’s view, to be incompetent is utter failure. Incompetency means one should be immediately replaced by someone with competency, because one doesn’t acquire competency overnight.
Again, I didn’t discuss Trump or the GOP with my dad but the incompetency doesn’t stop with RFK Jr.
It’s a mark of failure on every legislator who voted to approve RFK Jr. as Secretary of HHS in spite of his history of anti-vaccine propaganda and his lack of medical education. It’s a mark of failure on Trump for his nomination of RFK Jr., catering to the crunchy mom faction and the conditioned MAGA base, along satisfying the driver behind Russian influence operations which fed the anti-vaccine/anti-mask/anti-science faction.
Americans are going to die – some have already died – because of RFK Jr.’s incompetency. Some are becoming disabled and will become disabled because his incompetency doesn’t stop at throttling cancer and vaccine research, but undermining vaccine protocols and public health messaging.
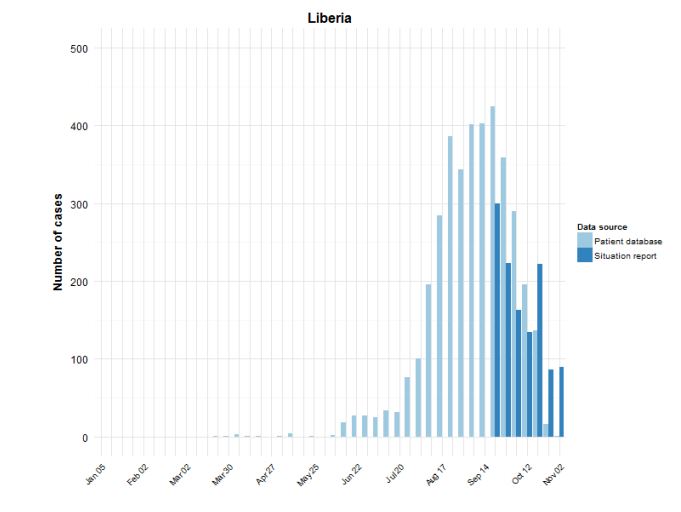
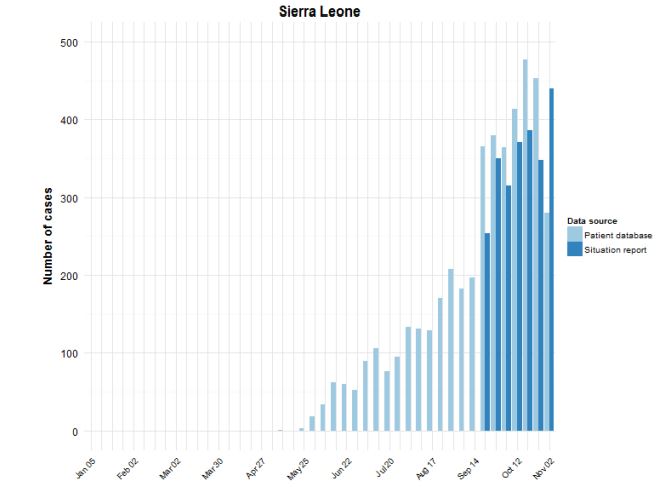
The explosion of measles and whooping cough cases, both of which had been managed by vaccines, will lead to greater numbers of disabled Americans. Measles has already killed at least three this year.
But vaccination numbers have dropped and continue to drop because the incompetent running HHS believes vaccines are somehow less safe than the diseases they prevent.
This same incompetent worm-eaten wackjob, approved by GOP legislators after nomination by a GOP president, has now ensured hope for immunotherapy and vaccines for disease like pancreatic cancer are throttled for at least the next three years.
Unless somehow GOP members of Congress catch a clue and realize national security includes the current and future health of this country, and investing in it with federal funding is essential, unless they catch a clue that a president with obvious age-related cognitive deficits is not the leader they should follow to assure the nation’s safety.
Unfortunately I won’t bet on this awakening during my father’s now-foreshortened lifetime.
__________
You can help Congress catch a fucking clue; call your members of Congress at (202) 224-3121 and demand they impeach RFK Jr. for incompetency. 5Calls.org also has a petition you can use to demand RFK Jr.’s impeachment.
Members of Congress are back in their state and district for the holiday break. You could also call the closest local office and find out if and when they are making public appearances at which you can demand they support impeaching the incompetent RFK Jr.