The Inaugural Donald J. Trump Awards
The Inaugural Donald J. Trump Award Trophy, awaiting the engraving of Donald J. Trump’s name and massive accomplishments.
It’s been quite a year, which is just the way Donald Trump, a narcissist the likes of which the world has never seentm, wants it.
Almost.
Can’t you just hear him: “I do, I do, and I do some more, more than anyone else ever, and yet I don’t get all the accolades I deserve. Haters.”
Now sure, he got the inaugural Gianni “Human rights problems? What human rights problems?” Infantino FIFA Peace Prize. But he wanted more, as he believes is only his due. Sadly, so many other awards have been somehow given to other clearly underdeserving folks, and still other awards are just begging to be given but no one has had the imagination or chutzpah to actually award them.
Until now. May I have the envelopes, please?
The Donald J. Trump Award for Narcissistic Rebranding goes to . . . Donald J. Trump for The Donald J. Trump and John F. Kennedy Center for the Performing Arts. And how dare any mere jazz musicians object to this.
The Donald J. Trump Award for Nationalistic Rebranding goes to . . . Donald J. Trump for the Gulf of America. All the haters at the AP and elsewhere can just get a life.
The Donald J. Trump Award for Interior Decoration goes to . . . Donald J. Trump for the over-the-top golden decorations, the “live, laugh, love” style signage, and the stunning — really absolutely stunning — renovations of the Lincoln Bathroom at the White House. The Presidential Walk of Fame with its image of Biden the AutoPen and the jawdropping plaques recounting each president’s achievements is truly beyond belief.
The Donald J. Trump Award for Architectural Salvage goes to . . . Donald J. Trump for his efforts to save the nation from the abomination that was the White House East Wing and replacing it with a much more appropriate Donald J. Trump White House Ballroom. Specific plans for the ballroom remain vague – I believe the phrase “we have a concept of a plan” fits this project, among others – but simply removing the East Wing was something that clearly needed to happen. And why does FLOTUS need any office space anyway?
The Donald J. Trump Award for Services to the Legal Community goes to . . . Donald J. Trump for his amazing record of presidential appointments to remake the legal system. From his SCOTUS appointments at the top to his appointment of judges like Emil Bove in the middle and Aileen Cannon at the bottom, as well as his appointment of prosecutors like Jeanine Pirro and Lindsey the Insurance Lawyer, he has truly installed only the best peopletm and that would be enough to earn him this award. But Trump didn’t stop there. Add to this the way in which he pushed out career DOJ staffers and the manner in which he got Big Law to bend the knee in the private sector, and this award is a slam dunk.
The Donald J. Trump Award for Medical Advancements goes to . . . Donald J. Trump for his efforts to dismantle and destroy the World Health Organization. Reading what Johns Hopkins University’s Bloomberg School of Public Health describes as WHO’s role in the world, it is obvious that WHO is a clear nuisance that needs to go:
The WHO plays many roles—the visible, apparent roles that many people are familiar with, and the roles that are less visible. This includes:
- Detecting, monitoring, and responding to emerging health threats, pandemics, and diseases of importance; we saw that during the COVID-19 crisis.
- Gathering and evaluating data and information from all over the world in order to understand the status of health globally and detect emerging problems. This includes acute crises as well as larger trends in health—which issues are causing a higher burden of disease and which ones we’re making progress on and should sustain efforts to address.
- Setting standards and developing guidelines that help people around the world, including here in the U.S., deal with various health threats and crises—not only infectious diseases, but all sorts of health issues.
- Providing commodities and goods to improve health around the world, including vaccines and drugs for many diseases. The U.S.’s withdrawal from WHO impacts not only the people who receive those goods, but also the supply chain for them, which includes many people in corporate America.
- Assisting with humanitarian response, which has important implications both for the populations who are affected by those crises and for global diplomacy and the role of our humanitarian responses in improving global diplomacy around the world.
- Providing very important technical assistance to governments and partners around the world to be able to respond to health challenges. The U.S. plays a very important role in providing this technical assistance.
Yeah. Who needs all that? (The “Bloomberg” in the name of the school was a clear giveaway as to JH’s unreliable wokeness.)
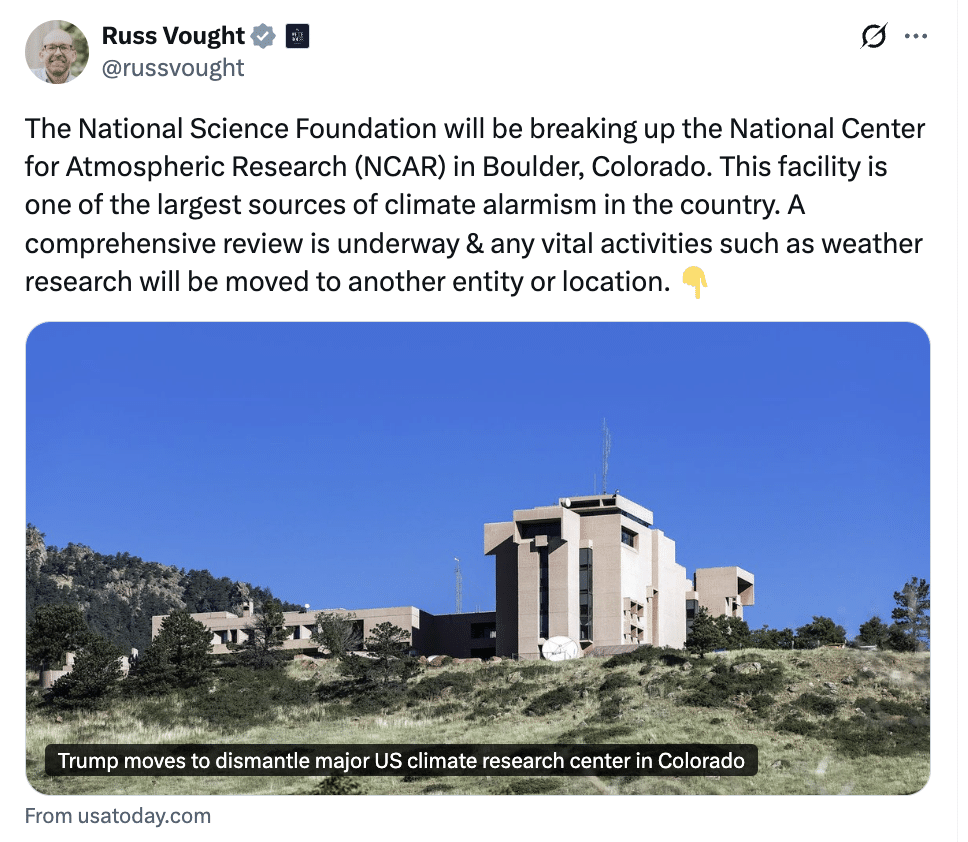
The Donald J. Trump Award for Services to the Environment goes to . . . Donald J. Trump’s decision to shut down the National Center for Atmospheric Research in Colorado. As climate scientist Kim Cobb told PBS,
“We’re talking about unique, one-of-a-kind facilities like supercomputers, ticked-out [sic, should be tricked-out] airplanes, and most importantly, a staff of over 800 people who are at the top of their game in innovating in weather and climate science for public good, putting out data that is on every single climate scientist’s computer around the country, if not around the world, and a nexus of collaboration as well that is important training grounds for the next generation of leaders.”
Yeah. Who needs all that when we’ve got The Weather Channel, amiright?
The Donald J. Trump Award for Service to Diplomacy goes to . . . Donald J. Trump for his muscular engagement with Nigeria, Venezuela, Iran, Yemen, Syria, Somolia, among other nations. (Simply renaming the US Institute of Peace as the Donald J. Trump US Institute of Peace seems hardly enough of a recognition for Trump’s breathtaking diplomatic work.)
The Donald J. Trump Award for Economic Excellence goes to . . . Donald J. Trump for his truly amazing grasp of the power of tariffs. Just ask the Kentucky Bourbon industry, US soybean farmers, and the members of the chambers of commerce in cities and towns along the US/Canada border.
The Donald J. Trump Award for Civil Rights goes to . . . Donald J. Trump for his dismantling of anything that smacks of a lack of racial harmony throughout American history. The Stonewall Riots, the Civil War, and anything having to do with Native Americans are merely the tip of the iceberg on the list of things that need to be forgotten, for the good of the nation. Trump is Making America Great Again by going back to the basics. As the faculty senate of Haskell Indian Nations University put it, Trump’s cuts to Native American education “represents a continuation of the trail of broken treaties” that is all too familiar to Native Americans. (Rumor has it he is working on how to get the women back in the kitchen (barefoot and pregnant), the gays back in the closet, and the blacks back in the fields, but those are clearly just rumors. I think. I hope.)
And that’s just a start.
I’m sure there are awards I am missing, but I trust that the imaginative and creative Emptywheel commentators can add to the list. Because really, Alfred Nobel has six prizes with his name on them, and what did he do, really, except invent dynamite? Trump surely deserves many more awards with his name on them than Nobel’s six. or the few that I have listed here.
Trump is truly in a league of his own.
Happy New Year’s, everyone. May next year be better (OK, that’s a low bar, but I’ll take it.).